







-

Physical Exam
Presented at the hospital with a fever and respiratory distress
Vital signs on presentation:
-

Hospital Course
Admitted into the hospital and received IV fluids and broad-spectrum antibiotics
- Chest X-ray was consistent with pneumonia of unknown etiology

On day 3, all cultures were NGTD except NP swab, which was positive for PIV.
-

Labs/Imaging
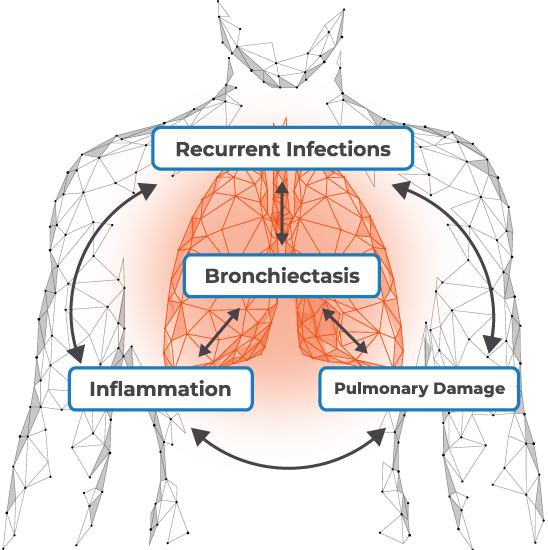
Chest CT scan revealed interstitial pneumonia with bronchiectasis
PaO2 = 65 mm Hg -

Follow-Up
One week after hospitalization, developed hypotension requiring vasopressors
CLICK HERE TO LEARN MORE ABOUT RVI TREATMENT GOALS AND STRATEGIES